When a doctor writes a prescription, a simple checkbox for "dispense as written" or "substitution permissible" can change the entire trajectory of a patient's treatment. While the FDA generally views generic drugs as interchangeable with brand-name versions, professional medical organizations aren't always on the same page. The tension lies between the undeniable economic benefit of lower-cost medication and the clinical fear that a tiny variation in a drug's formulation could lead to a medical crisis.
The Framework of Generic Standardization
To understand why medical societies take specific stances, we have to look at how these drugs are named and approved. Medical society guidelines is a set of formal positions established by professional medical organizations that influence clinical practice, prescribing patterns, and substitution policies. These guidelines didn't appear in a vacuum; they evolved alongside the Hatch-Waxman Act is the 1984 legislation that created the modern legal framework for generic drug approval in the United States . This law paved the way for the Abbreviated New Drug Application (ANDA) process, which allows generic makers to bypass repeating expensive clinical trials as long as they prove the drug is bioequivalent to the original.
A central player in this process is the United States Adopted Names Council, or USAN Council, operated by the American Medical Association (AMA). Their primary job isn't just labeling; it's safety. By standardizing nonproprietary names, they aim to reduce medication errors. If two drugs sound too similar, a pharmacist or nurse might grab the wrong vial. The USAN Council ensures that naming conventions are practical for healthcare providers, prioritizing suitability for routine prescribing and dispensing.
Where Specialists Disagree: The Case for Caution
If you ask a general practitioner about generics, they'll likely point you toward the cost savings. However, specialists often have a different perspective, especially when dealing with generic drug use in high-stakes scenarios. The most prominent example is the American Academy of Neurology (AAN), which officially opposes the generic substitution of anticonvulsant drugs.
Why the hesitation? It comes down to the Narrow Therapeutic Index (NTI). An NTI drug is one where the window between a dose that works and a dose that is toxic (or ineffective) is incredibly small. For the 3.4 million Americans living with epilepsy, a slight variation in how a generic drug is absorbed-even within the FDA's accepted 80-125% bioequivalence range-could be the difference between a stable day and a breakthrough seizure. For neurologists, the risk of a patient's seizure control failing outweighs the financial savings of a generic switch.

The Oncology Exception and Off-Label Use
In contrast to neurology, oncology has developed a more flexible approach to generics. The National Comprehensive Cancer Network (NCCN) provides guidelines that are widely used for Medicare coverage determinations. Interestingly, the NCCN Guidelines frequently incorporate off-label uses of generic drugs.
In the world of cancer treatment, the NCCN Compendia serves as a disease-specific roadmap. Because oncology often requires cutting-edge or repurposed therapies, about 42% of the drug uses listed by the NCCN are considered off-label. In this ecosystem, therapeutically equivalent generic products are often seen as equally safe and effective, allowing for a more seamless substitution process than what you'll find in neurology.
| Organization | General Stance | Primary Concern / Driver | Typical Drug Focus |
|---|---|---|---|
| AMA (USAN Council) | Supportive / Regulatory | Patient safety via nomenclature | All drug classes |
| AAN | Opposed (Specific) | Bioequivalence variations | Anticonvulsants (NTI) |
| NCCN | Supportive / Adaptive | Access to off-label therapies | Oncology medications |
| FDA | Strongly Supportive | Therapeutic equivalence | All approved generics |
The Gap Between Regulation and the Clinic
There is often a friction point between the Food and Drug Administration (FDA) and the actual clinical experience of a provider. The FDA maintains a firm stance: if a drug is rated "A" in the Orange Book (Approved Drug Products with Therapeutic Equivalence Evaluations), it is therapeutically equivalent. Period.
But doctors don't just treat data; they treat people. Clinical feedback suggests that while generic substitution rates hit nearly 90% across the board, a significant portion of specialists report complications. For example, some surveys indicate that up to 68% of neurologists believe generic antiepileptic substitutions have caused issues in their practice. This creates a legal and ethical gray area for pharmacists. In some states, laws require the pharmacist to get the prescriber's consent before substituting an NTI drug, while other states allow it freely. This inconsistency means a patient's medication safety might depend on their zip code.
Economic Pressures and Patient Access
We can't ignore the money. Generic drugs account for a staggering 90% of all prescriptions filled in the U.S., yet they only make up about 23% of total drug spending. This massive gap is why groups like the Generic Pharmaceutical Industry Association (GPIA) push for expanded substitution. They argue that generics make healthcare sustainable.
Medical societies are caught in the middle. On one hand, they want to lower the cost of care for their patients. On the other, they must defend the standard of care. When the USAN Council decides on a new drug stem, they have to consider if a name is too similar to an existing one. If they make a decision that makes a drug's name unappealing or confusing, it might actually discourage a company from developing a new medication, potentially cutting off patient access to a life-saving treatment.
Moving Toward a Unified Standard
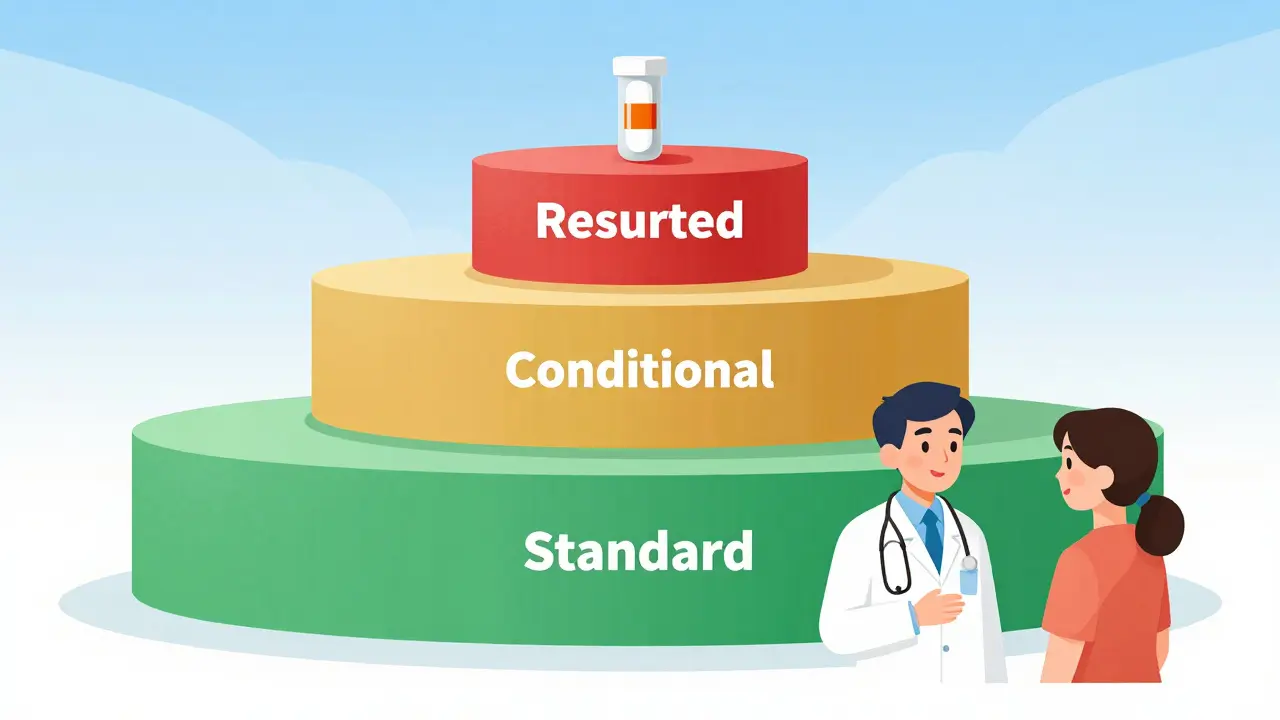
As we move further into 2026, the trend is toward tighter alignment with the FDA's therapeutic equivalence ratings. However, the "one size fits all" approach is fading. We are seeing a shift toward a tiered system of substitution:
- Standard Substitution: Most drugs (statins, blood pressure meds) follow the FDA's "A" rating and are swapped without hesitation.
- Conditional Substitution: Drugs where the provider may specify a brand or a specific generic manufacturer based on patient history.
- Restricted Substitution: High-risk NTI drugs where medical society guidelines (like those from the AAN) strongly advise against switching without a controlled transition.
For the patient, this means the conversation with the doctor is more important than ever. Asking "Is this a Narrow Therapeutic Index drug?" can be the key to ensuring the medication being dispensed is the exact one the physician intended.
Do all medical societies agree that generics are safe?
No. While most organizations align with the FDA's view on therapeutic equivalence, some specialty societies-like the American Academy of Neurology-express concerns about specific classes, particularly anticonvulsants, where minor variations in bioequivalence could trigger seizures.
What is the "Orange Book" and why does it matter?
The Orange Book is the FDA's official list of approved drug products with therapeutic equivalence evaluations. A rating of "A" means the generic is considered therapeutically equivalent to the brand-name drug, meaning it's generally expected to have the same clinical effect.
What does "Narrow Therapeutic Index" (NTI) actually mean?
NTI refers to drugs where there is a very small difference between the dose that is effective and the dose that becomes toxic. In these cases, even a small change in the blood concentration of the drug can lead to treatment failure or severe side effects.
Why does the NCCN allow off-label generic use?
Oncology often requires using drugs for conditions other than those specifically FDA-approved (off-label). The NCCN Guidelines provide a disease-specific compendium that helps providers use generic versions of these drugs safely and effectively to improve patient access and reduce costs.
Can a pharmacist change my brand-name drug to a generic without my doctor's okay?
In many cases, yes, if the drug is deemed therapeutically equivalent. However, this depends on state law and whether the doctor wrote "Dispense as Written" (DAW). For NTI drugs, some states specifically require prescriber consent before substitution.